
How not to save the economy? The interplay of economics and health during the COVID-19 pandemic

Exploring Economics, 2021
How not to save the economy? The interplay of economics and health during the COVID-19 pandemic
Authors: Vera Leuner, Navaneeth M S, Leandro Pereira Monteiro, Eduardo Lacerda Camargo Bisneto
Mentor and review: Dr. David Fasenfest
This is an essay that was created as part of the Rethinking Economics Sciences Po writing workshop "The Economics of the New Reality – Looking at the World Under the Pandemic from Pluralist Lenses", published in July 2021. It is a secondary data analysis combined with reflections on the empirical findings of other authors.
Summary
This article looks back at the beginning of the pandemic and explores the perceived trade-off between health and economy in the fight against COVID-19. Focusing on the different strategies adopted at the national level, we analyse the effects that the different intervention pathways had on the health of citizens and the economic performance of their countries. We propose that countries that fared better adopted similar strategies, which were guided by communitarian values, and put a preference on choosing health as a precondition for a healthy economy. Extending this discussion to the international level, the difficulties of obtaining global health within the current global framework are analyzed, underlining the statement that the pandemic isn’t over until it’s over everywhere.
1. Introduction
At the moment of writing, the global COVID-19 pandemic has already ravaged the entire world and a few countries are managing to overcome the virus through massive vaccination plans. If vaccines look like an attractive way out of the pandemic, how countries behaved in the early days was the subject of much more disagreement. In their national crisis response, most countries began thinking about the pandemic in a dichotomic manner: a trade-off between “lives versus livelihoods” (Schwab and Malleret, 2020). Albeit country-specific differences, the experience has shown that those who chose lives by implementing health measures targeted at eliminating the virus, also fared better economically in contrast to those who chose to bolster the economy.
Another layer is that, due to the global nature of pandemics, the policy choices made by each country have an impact on the rest of the world. For example, new variants emerging in countries where the virus is out of control to pose a risk to the creation of collective immunity through vaccines even in countries that had controlled the virus. Recognizing the importance of a coordinated global response, the World Health Organization (WHO) has supported national strategies to rapidly detect and respond to COVID-19 by providing technical information, coordinating health research, and raising emergency funds. Countries were advised by the WHO to pursue a strict elimination strategy. The benefits of such a strategy were later confirmed by the success stories of the pandemic. Nevertheless, many countries disregarded the recommendations and implemented different plans. Gathering the costs of not listening to the recommendations by the WHO at the national level and international levels, and providing potential explanations for this behaviour will be the contribution of this paper.
In the first part, this article aims to explore patterns in the strategies countries pursued from the start of the outbreak onwards. Afterwards, we explore the effects the different pathways had on the health of citizens and the economic performance of their countries. The third part focuses on how individual action, when it comes to a global issue like a pandemic, does not necessarily lead to an optimal collective outcome. The perceived best practices in the national interest can have nefarious consequences globally. Finally, we think about the capacities and constraints of the current global health governance system and add our conclusory remarks.
2. Worldwide patterns in reaction to the health crisis
Governments worldwide faced a choice about how to treat the virus early on in the pandemic. We find that countries followed either one of three different paths: the elimination strategy (or “zero-Covid”, “aggressive suppression”), the mitigation strategy to keep infections at a moderate level (or “stop-and-go”, “flattening the cure”), or accepting high numbers of severe cases by just protecting the persons most at risk (“herd immunity strategy”, officially planned and implemented only in Sweden, but might describe well the reality observed in many low-income countries) (Guangyu et al., 2021). In its Strategic Preparedness and Response Plan, the WHO, which had classified COVID-19 in the highest risk category (Guangyu et al., 2021), took a clear stance in advising countries to take up the aforementioned elimination strategy by identifying, diagnosing and treating cases (WHO, 2020).
Those adopting an elimination strategy, for example China, Australia, New Zealand, Taiwan, Vietnam, Japan, Korea, and Thailand, focused on controlling the virus early on with strict and smart containment measures, like early lockdowns, massive testing and modern contact tracing efforts, often mandatory isolation and treatment of cases in hospitals rather than at home, and a myriad of heterogeneous policies aimed at stopping outbreaks and contaminations, like restricting travel to prevent reimportation of the virus (Aghion et al., 2021; Guangyu et al., 2021). A growing literature shows the positive effect of accompanying hard measures like lockdowns with smart and early measures like testing in reducing deaths and economic downturns (Hosny, 2021).
On the other hand, we have the countries that chose to follow a mitigation strategy. Usually motivated by economic concerns, these countries faltered to take a hard stance on combating the virus and interrupting the chain of infection. Their strategy focused on reacting to the crisis once the conditions had deteriorated, thus, demanding more strenuous and long lockdowns which had a larger toll on the economy and health of its citizens. Besides, the constant opening and closing of the economy increased the level of instability and rendered private companies' planning useless (Aghion et al., 2021). The USA, UK, Brazil, and most European countries (including Germany, especially during the second wave) followed this strategy and registered worse numbers overall.
In the following chapter, we elaborate on the flawed rationale of the group of countries that chose mitigation. More precisely, it turned out that choosing to save the economy at the cost of the health of their citizens was a one-way street. Also, some of the underlying societal values and enabling factors that shaped the decision-making and the stringency of the taken measures are explored.
3. A flawed trade-off between economy and health
Were the concerns for the economic downturn by countries opting for the mitigation strategy justified? A first impulse when assessing the range of reactions at hand has been to weigh the costs of health policy measures against their use. Guided by the technique of economists’ “thinking at the margin” (Gans, 2020), there seems to be a real trade-off between human and economic health to be made. Intuitively, this holds true. The containment measures put in place by different countries around the world have had their toll on the economy. However, this thinking is short-sighted. Gans (2020) argues that pandemics have two characteristics that complicate the choice. Firstly, economic losses happen in a pandemic even without health policies in place. The strategy to let the virus “burn through” the population causes an economic loss at least via the deaths constituting a loss of workforce (ibid.). Thus, the choice for the economy will per se also contain economic losses. In addition, due to both shocks in aggregate supply and aggregate demand, pandemics cause economic recessions even in the absence of any containment measures (Eichenbaum, Rebelo, and Trabandt, 2020). Secondly, the critical moment of choice between economy and health is right after the outbreak of the pandemic. Because of the exponential transmission of COVID-19 a too long postponement of health measures can cause a “drift”, the moment when public health cannot be reached anymore - no matter the reduction in economic activity (Gans, 2020). Thus, the alternatives at hand and their costs vary strongly between the early and later stages of a pandemic. This describes well the situation countries like Brazil find themselves in currently.
Looking at the empirics of both health and economic costs, it becomes clear that the decision against eliminating the virus was detrimental to both of them. During the second quarter of 2020, the countries that recorded a better result in GDP growth when compared with the same period from 2019 were generally the ones who opted for an elimination strategy and, thus, had lower COVID-19 death rates (Hasell, 2020). Even though there are many factors determining the outcome of each government’s strategy, Hasell (2020) found no evidence that protecting people’s health was not also protecting the economy. The picture does not change much if the time frame is extended. Aghion et al. (2021) plot each one of the countries’ record for weekly deaths per million and weekly GDP change and their conclusion is similar. Not only did the countries that adopted an elimination strategy regain economic stability and growth faster than the ones that adopted the mitigation strategy, but they also suffered very few casualties related to the virus. These findings are also demonstrated in figure 1, in which selected countries are plotted. The mitigation strategy depicts high death rates and a deeper economic downturn with slower recovery. On the other hand, the successful cases of elimination were able to catch up with positive GDP growth (except Japan) and suffered substantially fewer deaths.
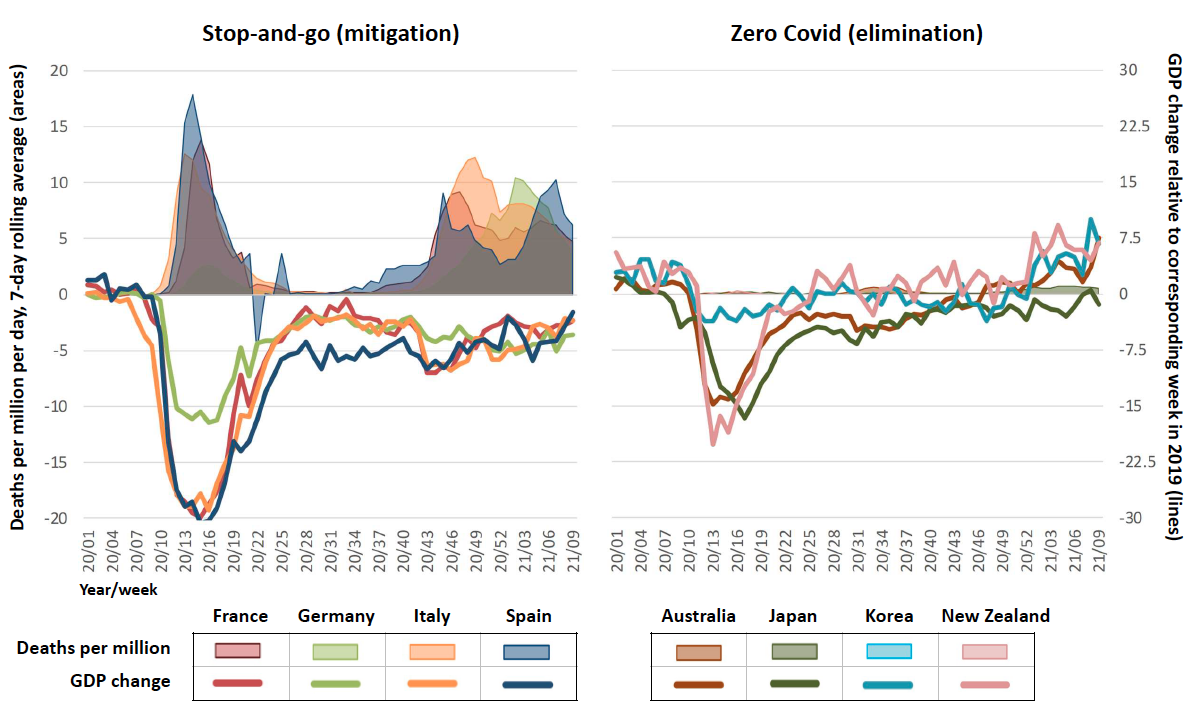
Figure 1: Mortality and GDP growth in selected countries
Taken from Aghion et al. (2021)
To which group each country belongs is determined by a deliberate choice of strategy by the governments and its speed of reaction. The pre-existent medical infrastructure and treatment capacity was not the determinant factor explaining how countries performed in relation to the pandemic. Low-scoring countries on the Global Health Security Index (2019), like Vietnam, managed to control the pandemic based on contact tracing and quick responsiveness. So did South Korea, a country with better infrastructure and treatment capacity. On the other hand, the USA, and the UK, which rank first and second in the Global Health Security Index (2019), respectively, suffered heavy losses both in lives and in GDP terms.
What, however, the countries that chose elimination have in common is the shared experience with previous outbreaks of coronavirus and a strong cohesiveness among communities, which however can also be attributed to varying degrees of social control (Guangyu et al., 2021). These factors provided the political will to contain and eliminate transmission at the early stages, no matter the cost. On the other hand, governments opting for the mitigation strategy lacked both the political will and the legitimacy to implement costly policy measures, paramount to save lives. An interesting case in this regard is Germany. While the first wave was controlled through early and broad testing and a still largely accepted lockdown between March and May 2020, the second wave in October was taken seriously only after health departments were close to exhaustion, and effective contact tracing and testing were virtually impossible (ibid.). The subsequent lockdowns announced in November, and mid-December were rather moderate and substantially less effective than the first one. Social cohesion and acceptance of lockdowns have been deteriorating (ibid.). Rallies against the COVID-19 measures in Germany demonstrate a missing “public willingness to sacrifice privacy for public health” (ibid.). Societal priorities regarding “lives vs livelihoods” among other factors could have made an elimination strategy impossible to implement.
Underlying values, some shaped by historical experiences, influenced whether prioritizing lives over short-term livelihood deterioration, inconvenience, and (a comparably low) economic loss was pursued. Prioritizing health policies was embedded in valuing the collective wellbeing and being able to draw back to a community response. Turning from the local to the global policy-making, we find similar frictions in the belief that a collective pull together is necessary for eliminating COVID-19.
4. Individual action against collective optimal outcomes
Looking at the behaviours of individuals and countries worldwide during the pandemic from a more philosophical perspective, we find that my decision as an individual or as a nation affects the whole society and world. This idea is well presented in the quote by philosopher Herbert Spencer “Your freedom ends where the freedom of others begins”. If one chooses as an individual to not take the COVID-19 vaccine, one will not just put oneself in danger but others, too. Nations should think and act as a global economy and society and not as individuals. In the following paragraphs, there are some arguments that endorse these thoughts. No country is an island; they are all linked in a global system.
Individual nations prioritising their own health systems is a logical response at the first glance. But there are multiple issues to this. Firstly, the global nature of the pandemic means if the Global South is left out from being immunized the virus would continue to spread and would manifest into new variants that could undermine the whole vaccine strategy. Secondly, the weakened public health system in the developing world could mean the susceptibility for the next pandemic is very high for the region. The integrated nature of the global economy means that a zero-sum approach to the pandemic would cause no good as the overall demand would remain low with continuous severe disruption in supply chains.
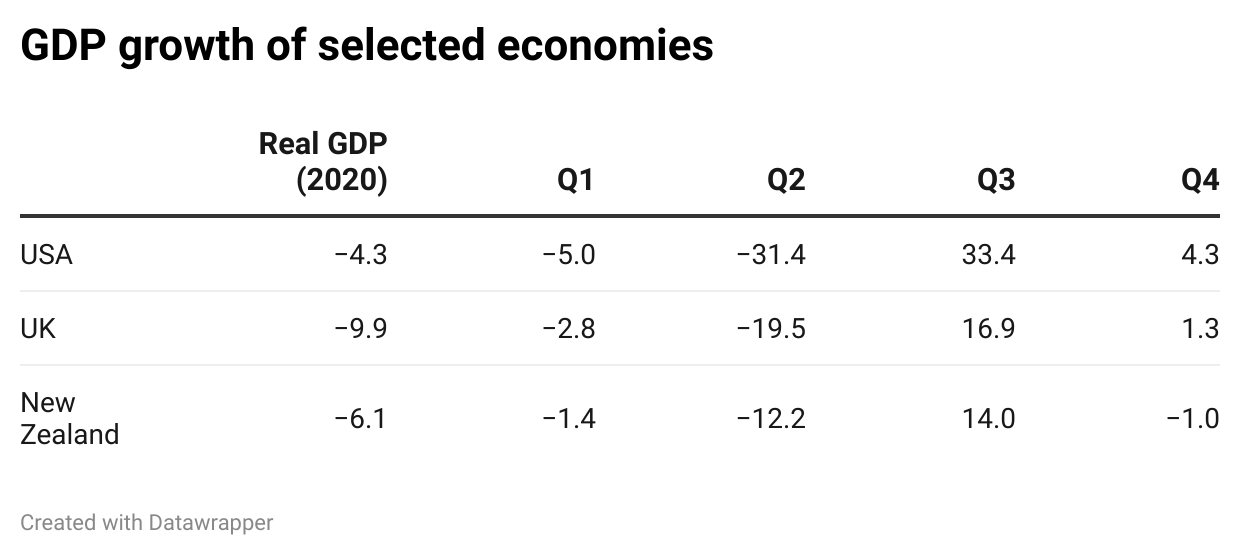
Table 1: The effect of Covid-19 across various economies
Source: IMF (2021)
As we can see from table 1, despite the successful handling of the COVID-19 crisis, New Zealand suffered a contraction in Q4 of 2020 due to the low recovery of its tourism and entertainment sector which is massively dependent on global footfall. This is despite its adequate handling of the pandemic and subsequent full-scale reopening of the economy. Many governments believe that they cannot depend on other nations, even close partners, in the current specific circumstance when it comes to the global public health crisis. It represents the classic case of ‘prisoner’s dilemma’ where two actors fail to cooperate since betraying the partner appears to offer a greater reward than cooperating in the short run (Hafner et al., 2020). One needs to further see this as part of the short-vision goals of most political leaders. While managing the pandemic needs a long-vision strategy and the benefits of which can only be seen at a date beyond their elected periods. This is also the reason why expenditure on public healthcare remains to be low especially in the developing world since sustained investment in the same is not a politically viable goal in the short run.
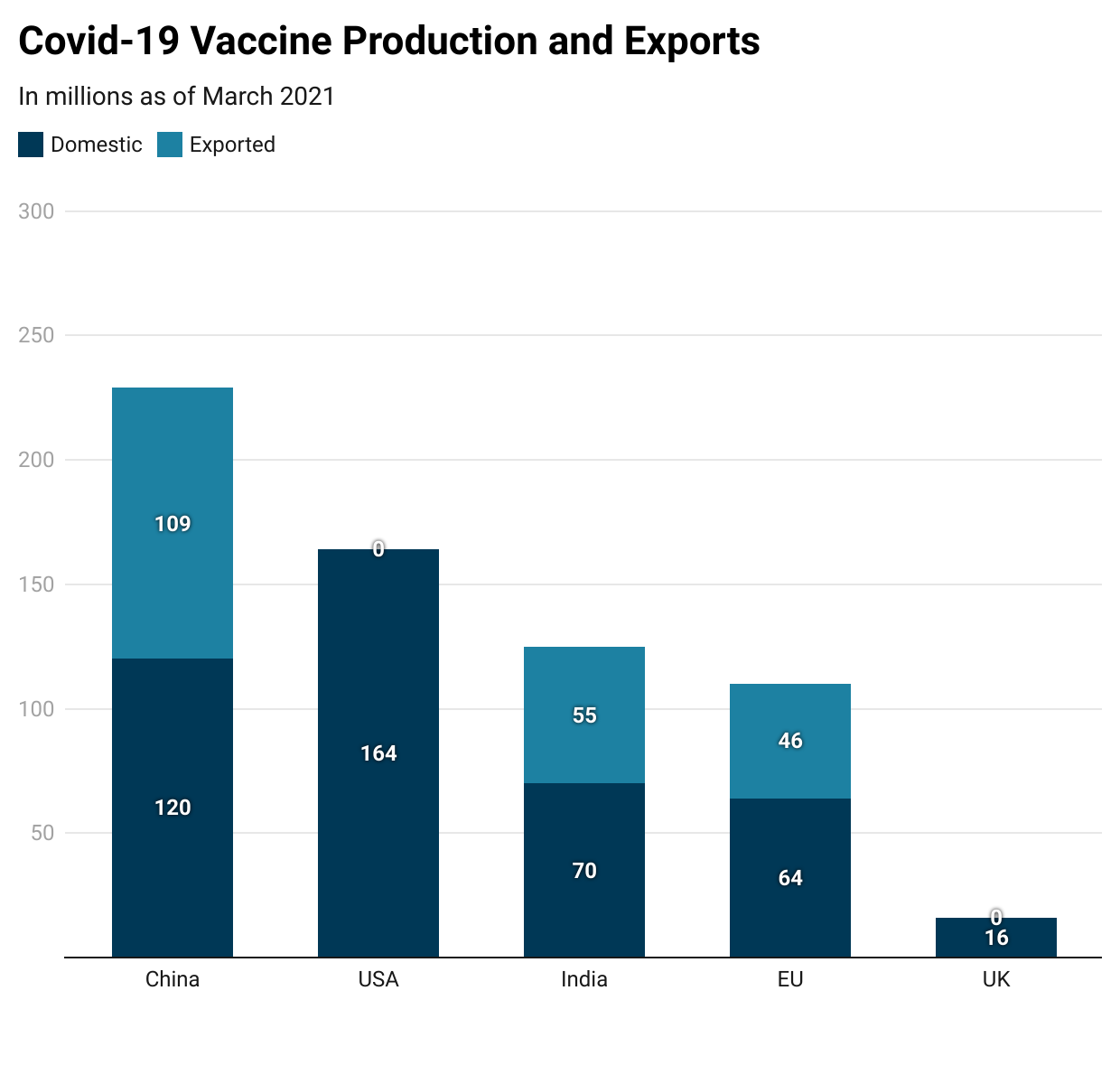
Fig 2: Global Vaccine Production
Source: Airfinty (2021)
When it comes to global issues, it's hard to have success with individual action given the divergence of multiple interests for a single agenda. Research on industrial innovation suggests the roadblocks that prevent cross-cultural collaboration and open innovation among various parties around the world are having multiple gatekeepers, scepticism with products being not invented at home, and turf wars (Deichmann, Rozentale and Barnhoorn, 2017). Individual actors are powerless to handle or monitor the mechanisms of institutional negotiation and the execution of the resulting regimes on their own. Analysis of environmental governance systems shows that institutional reductionism and overload are the two major reasons which determine a response strategy to be a success or failure. The former refers to the abstraction and simplification of the problem faced while the latter refers to the expansion of the scope of negotiation to the point that reaching an agreement is difficult or unlikely (Young and Stokke, 2020).
It is not new that eradicating a disease is good not just for the social and health outcomes of a country but also for its wealth. Studies conducted by Barret (2004) and Bloom et al. (2005) (Rodrigues, Plotkin 2020) show that eradicating the disease like smallpox cost 100 million USD but generated a saving of 1.35 billion USD and that polio elimination saved 1.5 billion USD annually. Similarly, the 2008 outbreak of measles in San Diego, triggered by an unvaccinated child, exposed almost 893 people and the subsequent quarantine and disease control measures cost the community close to 1 million USD (Sugarman et al., 2010).
Regarding the COVID-19 pandemic, similar estimations have been already made strongly proposing a full global recovery as the most economic solution. If wealthier nations are fully vaccinated, and the developing countries manage to vaccinate only half of their population, the resulting global economic loss will be around US$ 4 trillion (Selva et al., 2021). Even if the US, Europa, Japan and Canada vaccinate their whole population they will shoulder almost half the burden regarding the global trade loss (ibid.). As shown in a study called "Impact of vaccines; Health, Economic and Social Perspectives" (Rodrigues, Plotkin 2020) there is a 12% to 18% estimated investment return when provisioning vaccines from GAVI’s (Global Vaccine Alliance). The study also presents a monetary advantage of vaccination programs. For developed countries such as the United States the economic benefit is USD 69 billion per year and for Low- and Middle-Income Countries an investment of USD 34 billion would result in savings of USD 586 billion from the direct illness costs. A truly global vaccination rollout is not only ethically but also economically the most sensible solution.
5. Capacities and constraints of the global health system
As we have seen, the current state of affairs did not sustain the kind of collective coordination needed to efficiently fight the virus. Countries are more prone to act in their perceived best interest which can lead to different inefficient policies even if they have access to data and information indicating how to best respond to this crisis. When it comes to a collective issue with global implications, the aggregation of what was considered as being the optimal solution on an individual basis did not lead to an optimal outcome collectively. A way forward would be to embed the global health system in a sustainable culture that privileges a collective perspective on collective issues.
Nevertheless, the international institution best equipped to deal with global health threats and to coordinate international action to realize higher standards of health outcomes has been undermined during the pandemic. From nationalist threats to underfunding, there are multiple obstacles stopping the WHO from fulfilling its mandate. The pandemic has exposed WHO’s weakness when confronted with uncooperative member states. In theory, the WHO has significant powers and capacities. It is the only international body with the authority to declare a public health emergency of international concern (PHEIC), which allows for the issuance of nonbinding guidance on how to respond to the emergency. During a PHEIC, the WHO also emits guidelines for the treatment of diseases and coordinates global efforts in the fight against threats to global health security (CFR, 2021). On the other hand, the WHO is also equipped with a binding international law instrument, the International Health Regulations (IHR), which provides an overarching legal framework that defines countries’ rights and obligations in handling public health events and emergencies that have the potential to cross borders.
Albeit its different tools and capacities, several constraints impinge on the WHO’s ability to act effectively. First, it has a very low budget to fulfil its broad mandate. The lack of money can stop the WHO from providing global health governance and funding its different programmes and facilities. Besides, the WHO has become increasingly dependent on voluntary contributions, increasing its reliance on certain donors and its pervasiveness to political influence (CFR, 2021). Despite the budgetary shortcomings, the largest obstacle to collective success was the failure of the Member States’ responses and the lack of compliance with the IHR and WHO guidelines (Burwell and Townsend, 2020). The pandemic experience exposed Member State’s lack of commitment to international recommendations and WHO’s lack of authority to enforce them (ibid). Compliance with international rules or international organizations is a function of either coercion, self-interest, or legitimacy (Hurd, 1999). In the absence of coercive tools to enforce its decisions, bodies like the WHO need to rely either on the self-interest of international actors or on the normative belief that the rule is legitimate and, therefore, ought to be obeyed (ibid). As we have seen, leaving States to act based on their self-interest did not help achieve collective well-being. In its turn, legitimacy as a means of exerting social control also seems to be lacking in the international rules and institutions of global health.
Exploring how we could improve the global health order and WHO’s legitimacy goes beyond the scope of this paper, but it is useful to propose a starting point. Critical junctures like the COVID-19 pandemic can be perceived as an opportunity to reset the current state of affairs and build a better institutional framework for the future. Arguably, COVID-19 as an exogenous crisis can become a turning point in ending the already weakened neoliberal long wave (Kiliç, 2020). For instance, a post-colonial perspective allows for the critical examination of the sources of global health inequalities allowing reform to take place (Büyüm et al., 2020). Understanding the global health agenda as ignorant of how health risks are shaped structurally by geopolitical determinants and inequalities derived from neoliberalism is paramount to the process of transformation and improvement of the system that marginalizes a large proportion of the world’s population. Bringing the marginalized to the table might increase WHO’s legitimacy and overall respect for its authority. Now, it remains to be seen whether international actors are willing to answer this solidarity call to action in a fruitful and truly global manner.
6. Conclusion
In this paper, we have argued that there was a salient option between the strategies in fighting the Covid-19 pandemic. The elimination strategy recommended by the WHO achieved better results when it comes to saving both health and the economy. In our analysis, we mentioned different factors that could have contributed to the different outcomes but focused on the contrast between the strategies. We have attempted to show that both at the national and international levels opting for an individual take on the crisis is neither efficient nor realistic since we live in an interconnected world and the pandemic itself has a global nature. Finally, we looked at how present global health governance ends up constraining global responses to this sort of emergency.
Learning from past experiences is important to better prepare the world health system for the next pandemics, which are likely to happen more frequently (Patrick, 2020). Nonetheless, instead of pushing us to better and universal health governance, the critical juncture created by the pandemic might be leading us to a more fragmented nonuniversal system that resembles a multipolar club model (Gostin et al., 2020). By fragmenting the system even more, we risk diminishing global solidarity and increasing inequalities. Since we live in a globalized world, with fragmented production, global value chains, and so forth, it does not make sense to limit health access to national boundaries or clubs if health issues are fundamentally collective. In this scenario, the legitimacy of international organizations like the WHO needs to be reinforced to ensure its authority when leading a collective and solidary response.
References
Aghion, P., Artus, P., Oliu-Barton, M., Pradelski, B. (2021). Aiming for zero Covid-19 to ensure economic growth. Vox EU [online]. Available at: https://voxeu.org/article/aiming-zero-covid-19-ensure-economic-growth
Airfinity (2021). America First? Covid-19 Vaccine Production & Exports. Retrieved April 25, 2021, from: https://www.statista.com/chart/24555/vaccine-doses-produced-and-exported/
Burwell, S. M. and Townsend, F. F. (chairs) (2020). Improving Pandemic Preparedness: Lessons From COVID-19. Independent Task Force Report No.78. New York, USA: Council of Foreign Relations. Available at: https://www.cfr.org/report/pandemic-preparedness-lessons-COVID-19/pdf/TFR_Pandemic_Preparedness.pdf
Büyüm, A. M., Kenney, C., Koris, A., Mkumba, L., and Raveendran, Y. (2020) Decolonising global health: if not now, when?. BMJ Global Health, 5. DOI:10.1136/bmjgh-2020-003394
Cem, Ç., Selva, D., Sebnem, K., Sevcan, Y., & MUhammed, A (2021). The Economic Case for a global Vaccination An Epidemiological Model With International Production Networks. National Bureau of Economic Research. Cambridge MA.
CFR Editors. (2021). What Does the World Health Organization do?. Council of Foreign Relations [online]. Available at: https://www.cfr.org/backgrounder/what-does-world-health-organization-do
Cummings, M. (2020). Politics affect public buy-in On Covid-19 vaccine, study shows. Retrieved April 18, 2021. Available at: https://news.yale.edu/2020/10/27/politics-affect-public-buy-covid-19-vaccine-study-shows
Deichmann, D., Rozentale, I. and Barnhoorn, R., 2017. Open Innovation Generates Great Ideas, So Why Aren’t Companies Adopting Them?. [online] Harvard Business Review. Available at: https://hbr.org/2017/12/open-innovation-generates-great-ideas-so-why-arent-companies-adopting-them
Eichenbaum, M., Rebelo, S., Trabandt, M. (2020). The trade-off between economic and health outcomes of the COVID-19 epidemic. Vox EU [online]. Available at: https://voxeu.org/article/trade-between-economic-and-health-outcomes-covid-19-epidemic
Gans, J. (2020). Economics in the Age of COVID-19. MIT Press.
Global Health Security Index (2019) [online]. Available at: https://www.ghsindex.org/report-model/
Gostin, L. O., Moon, S., and Meier, B. M. (2020). Reimagining Global Health Governance in the Age of COVID-19. American Journal of Public Health, 110(11) [online]. Available at: https://ajph.aphapublications.org/doi/ref/10.2105/AJPH.2020.305933
Guangyu Lu, Oliver Razum, Albrecht Jahn, Yuying Zhang, Brett Sutton, Devi Sridhar, Koya Ariyoshi, Lorenz von Seidlein & Olaf Müller (2021). COVID-19 in Germany and China: mitigation versus elimination strategy, Global Health Action, 14:1.
Hafner, M., Yerushalmi, E., Fays, C., Dufresne, E. and Stolk, C., 2020. COVID-19 and the cost of vaccine nationalism. [online] Santa Monica, CA: RAND Corporation.
Hasell, J. (2020). Which countries have protected both health and the economy in the pandemic?. Our World in Data [online]. Available at: https://ourworldindata.org/covid-health-economy
Hosny, A. (2021). The sooner (and the smarter), the better: COVID-19 containment measures and fiscal responses1. Covid Economics, 137.
Hurd, I. (1999). Legitimacy and Authority in International Politics. International Organization, 53(2), 379-408.
Kiliç, S. (2020). Does COVID-19 as a Long Wave Turning Point Mean the End of Neoliberalism?. Critical Sociology, December 2020. DOI:10.1177/0896920520980083
Patrick, S. M. (2021). ‘Four Lessons From a Painful Pandemic Year’, World Politics Review, March 29 [online]. Available at: https://www.worldpoliticsreview.com/articles/29527/four-lessons-for-the-future-of-pandemic-disease
Rodrigues, C., & Plotkin, S. (2020). Impact of Vaccines; health, economic and social perspectives.
Schwab, K., & Malleret, T. (2020). The Great Reset. World Economic Forum, Geneva.
Sugerman, D., Barskey, A., Delea, M., Ortega-Sanchez, I., Bi, D., Ralston, K., Rota, P., Waters-Montijo, K. and LeBaron, C., 2010. Measles Outbreak in a Highly Vaccinated Population, San Diego, 2008: Role of the Intentionally Undervaccinated. PEDIATRICS, 125(4), pp.747-755.
Ward, J., Alleaume, C., & Peretti-Watel, P. (2020). The French Public's attitudes to a FUTURE Covid-19 Vaccine: The politicization of a public health issue.
World Health Organization (2020). COVID‑19 STRATEGY UPDATE. Geneva.
Young, O. and Stokke, O., 2020. Why is it hard to solve environmental problems? The perils of institutional reductionism and institutional overload. International Environmental Agreements: Politics, Law and Economics, 20(1), pp.5-19.